Autologous Facial Grafts Versus ePTFE Implants
Challenging Traditional Paradigms in Facial Augmentation
Introduction
For more than half a century, autologous tissue has represented the cornerstone of facial reconstruction and augmentation. The reconstructive principle of “replace like with like” has shaped generations of plastic surgeons and remains deeply embedded in contemporary surgical training. Whether performing dorsal augmentation rhinoplasty, malar reconstruction, mandibular augmentation, or correction of congenital facial asymmetries, cartilage, bone, fascia, and fat harvested from the patient have traditionally been regarded as the benchmark against which all alloplastic materials are measured.¹–³
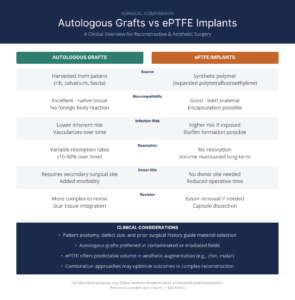
The rationale is compelling. Autologous tissue is biologically compatible, capable of incorporation into surrounding tissues, and free from concerns regarding foreign-body reactions or implant rejection. In complex reconstructive surgery involving irradiated tissue, composite defects, or vascularized tissue transfer, autologous reconstruction remains the unquestioned standard of care.²
However, contemporary facial surgery encompasses far more than reconstruction. Increasingly, surgeons are asked to perform highly precise contour modifications in otherwise healthy patients seeking aesthetic enhancement or correction of subtle skeletal deficiencies. The goals of these procedures differ fundamentally from those of reconstructive surgery. Rather than replacing missing tissue, the objective is often to restore balance, improve projection, or refine facial proportions with predictable, durable results.
These evolving indications have prompted renewed interest in modern alloplastic materials, particularly expanded polytetrafluoroethylene (ePTFE). Introduced into facial surgery more than three decades ago, ePTFE has accumulated an extensive clinical history demonstrating excellent biocompatibility, favorable soft-tissue integration, long-term dimensional stability, and acceptable complication rates when appropriately selected and meticulously implanted.¹,⁴–⁶
Today, commercially available ePTFE implants occupy an important place within the reconstructive armamentarium. Unlike earlier generations of synthetic implants, these materials possess a unique microporous architecture that permits controlled fibrovascular ingrowth while preserving the ability to revise or remove the implant when clinically indicated.¹,⁴ Among contemporary ePTFE implant options, Surgiform® implants are designed to leverage these material characteristics while providing surgeons with a range of reconstructive and aesthetic applications.
Perhaps most importantly, recent systematic reviews evaluating facial implant materials have failed to demonstrate convincing evidence that any single material is universally superior across all clinical indications. Rather, successful outcomes appear to depend on thoughtful patient selection, meticulous surgical technique, and matching the biomaterial to the reconstructive objective.⁷
Accordingly, the question facing today’s facial surgeon is no longer whether autologous tissue remains valuable—it unquestionably does—but whether it should continue to be viewed as the default solution for every facial augmentation procedure.
This article explores that question by comparing autologous grafts and ePTFE implants from the perspective of contemporary facial plastic surgery, emphasizing clinical decision-making rather than historical preference.
The Evolution of Facial Augmentation Materials
Facial implant technology has evolved considerably over the past four decades. Early alloplastic materials were frequently associated with migration, encapsulation, extrusion, or poor long-term integration. These experiences understandably reinforced the perception that autologous tissue represented the safest and most reliable option.
Modern biomaterials, however, differ substantially from their predecessors.
Expanded polytetrafluoroethylene possesses an interconnected node-and-fibril microstructure that allows limited fibrovascular ingrowth without extensive osseointegration. This unique biological behavior distinguishes ePTFE from both smooth silicone implants and highly porous polyethylene implants such as Medpor®.¹,⁴
Rather than behaving as an inert foreign body, ePTFE develops controlled soft-tissue incorporation sufficient to stabilize implant position while maintaining relative flexibility during future revision surgery. This intermediate biological response has become one of the defining characteristics of the material.
Consequently, the modern discussion should not be framed as autologous versus alloplastic, but rather as selecting the most appropriate biomaterial for a specific reconstructive objective.
The Hidden Cost of Autologous Tissue
The greatest strength of autologous grafting is also one of its greatest limitations: every graft must first be harvested.
While donor-site surgery has become routine for reconstructive surgeons, it introduces a second operative field with its own inherent morbidity. Costal cartilage harvest may be associated with postoperative pain, chest wall scarring, contour deformity, prolonged recovery, and the rare but significant risk of pleural violation. Harvest of calvarial bone introduces concerns regarding contour irregularity, dural injury, and additional operative complexity, while iliac crest grafting may produce postoperative discomfort that exceeds pain at the recipient site.²,³
Although these risks are generally acceptable in complex craniofacial reconstruction, they warrant greater consideration in elective facial augmentation where the procedure is intended to improve contour rather than restore missing tissue.
Equally important is the increased operative burden associated with autologous reconstruction. Tissue harvest, donor-site closure, graft preparation, contour refinement, and recipient-site implantation each contribute to longer operative times and greater technical variability.
In contrast, ePTFE eliminates donor-site morbidity entirely.
While this advantage is sometimes dismissed as merely a matter of convenience, avoiding a second operative site represents a meaningful reduction in cumulative surgical trauma. In aesthetic surgery, where minimizing morbidity is often a primary objective, elimination of donor-site surgery should be viewed as a legitimate clinical benefit rather than a secondary consideration.
Biological Tissue Does Not Necessarily Mean Biological Stability
One of the most persistent assumptions in facial reconstruction is that biologic tissue provides inherently superior long-term stability.
In reality, autologous grafts remain biologically active after implantation and therefore continue to undergo remodeling. Cartilage may warp, bone may partially resorb depending upon recipient-site vascularity and mechanical loading, and fat grafts remain susceptible to variable long-term survival despite continued advances in harvesting and processing techniques.²,³,⁸
Although these biological responses are often modest, they introduce an element of unpredictability that can complicate procedures requiring precise contour modification.
This issue becomes particularly relevant in modern aesthetic facial surgery, where surgeons frequently seek millimeter-level adjustments involving the pyriform aperture, infraorbital rim, malar eminence, prejowl sulcus, mandibular angle, or nasal dorsum.
In these settings, predictable dimensional stability becomes increasingly important.
Unlike autologous tissue, ePTFE is not subject to biologic resorption or remodeling. The contour achieved at implantation remains largely unchanged over time, allowing surgeons to achieve highly reproducible skeletal augmentation.¹,⁴,⁵
This stability should not be interpreted as evidence of superiority in every circumstance. Rather, it illustrates an important principle:
Living tissue and stable contour are not synonymous objectives.
In reconstructive surgery, biological incorporation may be paramount.
In contour augmentation, dimensional predictability may be equally valuable.
Recognizing this distinction represents one of the most important shifts in contemporary facial augmentation philosophy.
Autologous Tissue Remains the Standard—But Not the Default
None of these observations diminish the remarkable value of autologous reconstruction. There remain numerous clinical scenarios in which autologous tissue is unquestionably the preferred reconstructive option.
- Large composite defects following oncologic resection.
- Irradiated recipient beds.
- Complex craniofacial trauma.
- Congenital skeletal deficiencies requiring structural reconstruction.
- Procedures requiring vascularized tissue transfer.
In these circumstances, no currently available implant material can replicate the biological capabilities of living tissue. However, many facial augmentation procedures address an entirely different clinical problem. The surgeon is not replacing missing tissue. The surgeon is modifying contour. When augmentation rather than regeneration becomes the primary objective, the theoretical biological advantages of autologous tissue become less absolute.
This distinction forms the foundation for reconsidering the role of modern ePTFE implants within facial plastic surgery. Rather than asking whether autologous tissue is universally superior, a more appropriate question is:
Which material best solves the specific reconstructive problem while minimizing overall patient morbidity?
That question increasingly defines contemporary facial augmentation and sets the stage for a more nuanced discussion of implant integration, revision surgery, operative efficiency, and complication profiles.
Integration Versus Reversibility: Finding the Optimal Balance
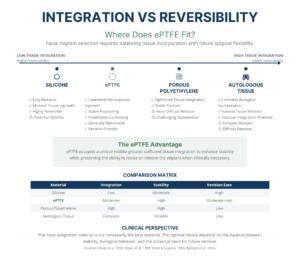
Historically, facial implant materials have often been categorized simply as either autologous or alloplastic. In reality, individual biomaterials differ considerably in their biological behavior, particularly with respect to tissue integration and the ability to perform revision surgery.
At one end of the spectrum, smooth silicone implants undergo relatively little tissue attachment. This characteristic facilitates straightforward removal or repositioning but may also contribute to implant mobility or capsule formation. At the opposite end, porous polyethylene (Medpor®) permits extensive fibrovascular ingrowth that provides excellent long-term fixation but may significantly complicate explantation or revision because of the intimate incorporation of surrounding soft tissue into the implant architecture.¹,⁴
Expanded polytetrafluoroethylene occupies a unique position between these extremes.
The microporous node-and-fibril architecture of ePTFE permits limited fibrovascular ingrowth while preserving implant flexibility and relative ease of revision. Histologic investigations have demonstrated soft-tissue incorporation with minimal chronic inflammatory response, allowing the implant to remain stable without becoming so extensively integrated that subsequent modification becomes prohibitively difficult.¹,⁴
This balance between biological incorporation and surgical reversibility is one of the defining characteristics of ePTFE and represents an important consideration in facial aesthetic surgery, where revision procedures are not uncommon.
Revision Surgery Should Influence Initial Material Selection
Unlike many reconstructive procedures, facial aesthetic surgery frequently involves patients whose anatomy, aging process, or aesthetic preferences evolve over time. Consequently, revision surgery should not be viewed as evidence of failure but rather as an anticipated possibility during long-term patient care.
This reality should influence implant selection from the outset.
Autologous grafts that have successfully incorporated into surrounding tissues often become technically challenging to modify. Secondary contour refinement may require extensive dissection, additional graft harvest, or partial graft removal, each introducing additional operative morbidity. Cartilage grafts may also undergo warping or subtle remodeling that necessitates delayed correction.²,⁸
By comparison, the controlled fibrovascular integration characteristic of ePTFE frequently permits relatively straightforward implant modification or removal when clinically indicated. Although revision surgery is never trivial, preservation of a defined implant plane can simplify secondary procedures while maintaining excellent implant stability during the intervening years.¹,⁴
For surgeons performing elective facial augmentation, revision potential should therefore be considered an inherent material characteristic rather than an afterthought.
Operative Efficiency Has Clinical Value
Discussions regarding operative efficiency are sometimes dismissed as primarily economic considerations. However, shorter, less complex operations may also benefit patients through reduced anesthesia exposure, elimination of donor-site surgery, and decreased cumulative tissue trauma.
Autologous grafting requires tissue harvest, donor-site closure, graft carving, contour refinement, repeated intraoperative adjustments, and implantation. Each additional step introduces opportunities for variability while extending operative duration.
By contrast, ePTFE implants may be selected, sculpted, and implanted without creating a second operative field. Implant preparation is reproducible, contour modification is efficient, and unlimited implant material is immediately available throughout the procedure.
Although operative efficiency alone should never determine implant selection, it represents another meaningful variable that contributes to overall patient morbidity.

Complication Profiles: Different Rather Than Better
One of the most common misconceptions in discussions comparing autologous tissue with alloplastic implants is the assumption that one material possesses an inherently superior safety profile.
However, the available literature suggests a more nuanced conclusion. These materials simply fail differently. Autologous cartilage avoids implant-specific complications such as extrusion or foreign-body infection but introduces donor-site morbidity, biological remodeling, tissue availability limitations, and graft-specific complications including warping and resorption.
A meta-analysis by Wee and colleagues evaluating 491 patients undergoing rhinoplasty with autologous costal cartilage demonstrated pooled complication rates of 3.08% for warping, 0.22% for resorption, 0.56% for infection, 0.39% for displacement, 5.45% for hypertrophic chest scarring, and an overall revision rate of 14.07%.⁸
These findings reinforce the excellent overall safety profile of autologous rib cartilage while simultaneously illustrating that donor-site morbidity and biologic variability remain important clinical considerations.
The complication profile of ePTFE differs substantially. Rather than warping or resorption, surgeons must consider infection, exposure, extrusion, contour irregularity, implant visibility, and occasional implant removal.
In one of the landmark clinical series, Godin and colleagues reported only three infections requiring implant removal among 137 augmentation rhinoplasty patients, corresponding to an infection rate of approximately 2.2% over six years of clinical experience.⁵ Similarly, Flowers reported infection in 5 of 200 ePTFE implants (2.5%) placed for augmentation of deep nasolabial folds, with elective removal in several patients because of excessive superficial contour rather than infection alone.⁹
More recently, a systematic review evaluating 117 studies involving more than 4,200 patients undergoing facial implantation reported an overall implant-related infection or inflammatory complication rate of approximately 1% across all alloplastic facial implants. Importantly, the authors concluded that available evidence remains limited by retrospective study design, inconsistent outcome reporting, and substantial heterogeneity, making direct comparisons between implant materials difficult.⁷
Perhaps the most important observation emerging from these studies is that no facial implant material demonstrates universally superior outcomes across all clinical situations. Instead, complication profiles should be interpreted within the context of the reconstructive objective. Autologous tissue introduces donor-site morbidity in exchange for biologic incorporation. ePTFE eliminates donor-site surgery while accepting the possibility of implant-specific complications.
The question is therefore not which material is safer in the abstract, but which complication profile is more acceptable for the individual patient and clinical indication.
The Infection Narrative Deserves Reconsideration
For decades, infection has remained the principal criticism of alloplastic facial implants. While foreign materials unquestionably introduce unique microbiological considerations, contemporary evidence suggests that postoperative infection depends far more upon operative technique than implant composition alone. Successful implantation requires meticulous pocket dissection, atraumatic soft-tissue handling, complete hemostasis, elimination of dead space, tension-free closure, and careful patient selection.
When these principles are followed, modern clinical series have demonstrated consistently low infection rates with ePTFE implants.⁵–⁷ This observation is supported by more recent reviews emphasizing biofilm prevention through meticulous surgical technique rather than reliance upon implant material alone.¹⁰ An additional consideration unique to ePTFE involves implant preparation immediately before insertion.
Because expanded polytetrafluoroethylene is intrinsically hydrophobic, many experienced facial plastic surgeons prepare implants using vacuum impregnation with an antibiotic or antiseptic solution prior to implantation. Laboratory investigations have demonstrated that vacuum impregnation significantly reduces bacterial contamination throughout the porous architecture of both implant types, providing a compelling mechanistic rationale for the technique.¹¹ However, no prospective clinical studies have yet demonstrated that vacuum impregnation independently reduces postoperative infection rates. Consequently, while the technique is biologically plausible and supported by laboratory evidence, it should presently be regarded as an evidence-informed adjunct rather than a proven method of reducing implant infection.
Ultimately, the available literature consistently supports a common conclusion:
Meticulous surgical technique remains the single most important factor influencing postoperative infection regardless of implant material.
This conclusion applies equally to autologous tissue and modern ePTFE implants and underscores the importance of thoughtful surgical planning over adherence to historical assumptions.
Precision Augmentation Favors Predictable Materials
One of the fundamental questions in facial augmentation is whether the surgical objective is tissue replacement or contour enhancement. Although these goals are frequently discussed together, they represent distinctly different reconstructive problems.
In reconstructive surgery following trauma, oncologic resection, or congenital deformity, the surgeon often seeks restoration of both anatomy and biologic function. Under these circumstances, autologous tissue offers advantages that no current alloplastic material can fully reproduce. Vascularity, biologic remodeling, and long-term integration remain critical to successful reconstruction.²,³
Conversely, many contemporary aesthetic procedures seek only to improve skeletal definition or facial proportion. Pyriform aperture augmentation, infraorbital rim augmentation, malar enhancement, mandibular angle augmentation, prejowl correction, and dorsal nasal augmentation frequently involve otherwise healthy tissues with adequate soft-tissue coverage. In these procedures, the primary objective is not biologic replacement—it is stable, reproducible contour enhancement. For these indications, the advantages of ePTFE become increasingly relevant.
Because ePTFE maintains its dimensions over time and is available in unlimited quantity, surgeons can achieve highly reproducible contour modifications without concerns regarding donor-site morbidity or biologic remodeling. The material is easily sculpted intraoperatively and can be layered or trimmed to achieve precise correction of localized skeletal deficiencies.¹,⁴,⁵ This predictability has contributed to the continued use of ePTFE in facial augmentation despite the availability of numerous alternative biomaterials.
Rather than viewing autologous tissue and ePTFE as competing philosophies, they should be viewed as complementary solutions designed to address different reconstructive objectives.

Material Selection Should Be Individualized Rather Than Ideological
Perhaps the greatest lesson from the contemporary facial implant literature is that material selection should be individualized rather than ideological.
For many years, discussions surrounding facial implants have centered on identifying the single “best” material. But, current evidence suggests that this question may be fundamentally flawed. Each biomaterial possesses unique biological, mechanical, and surgical characteristics that make it particularly well suited for specific clinical scenarios.
Autologous tissue remains the preferred option when the reconstructive problem requires living tissue capable of vascular incorporation and biologic remodeling. Large composite defects, irradiated recipient beds, major craniofacial trauma, and extensive congenital deformities continue to represent ideal indications for autologous reconstruction.²
In contrast, many elective facial augmentation procedures emphasize contour precision, procedural efficiency, donor-site avoidance, and the possibility of future revision. Under these circumstances, ePTFE offers several meaningful advantages:
- Elimination of donor-site morbidity
- Excellent dimensional stability
- Controlled fibrovascular integration
- Unlimited material availability
- Simplified intraoperative contouring
- Relative ease of revision or removal when compared with more extensively integrated implants¹,⁴–⁷
The decision therefore should not be framed as autologous versus ePTFE, but rather as which material best addresses the clinical problem while minimizing overall patient morbidity.
This subtle shift in thinking reflects the maturation of facial implant surgery over the past three decades.
Looking Beyond Historical Dogma
Plastic surgery has always evolved through thoughtful reassessment of established practices. Numerous techniques once considered controversial—including microvascular free tissue transfer, endoscopic facial surgery, fat grafting, and patient-specific implants—have ultimately become accepted components of contemporary reconstructive surgery because surgeons remained willing to question historical assumptions while carefully evaluating emerging evidence.
The discussion surrounding ePTFE facial implants deserves similar consideration. The available literature does not suggest that ePTFE should replace autologous tissue. Nor does it suggest that autologous reconstruction has become obsolete.
Rather, contemporary evidence supports a more balanced conclusion:
- Both materials possess important advantages.
- Both possess limitations.
- Neither should be considered universally superior.
Instead, surgeons should continue selecting implant materials according to the biological requirements of the reconstructive problem, the characteristics of the recipient site, anticipated revision requirements, patient preferences, and their own clinical experience.
This represents a more sophisticated and evidence-based philosophy than simply defaulting to autologous tissue whenever possible.
Conclusion
Autologous facial grafts have earned their place within facial plastic and reconstructive surgery through decades of reliable clinical performance. Their biological compatibility, capacity for incorporation, and proven reconstructive success ensure that they will remain indispensable for many complex facial procedures.
However, facial augmentation has evolved considerably.
Modern aesthetic surgery increasingly emphasizes precision contouring, predictable long-term stability, reduced operative morbidity, and efficient revision when necessary. Within this context, expanded polytetrafluoroethylene has emerged as a highly effective biomaterial that addresses many of the limitations associated with autologous grafting while maintaining an excellent safety profile when used appropriately.¹,⁴–⁷
Current evidence suggests that the historical perception of autologous tissue as the universal “gold standard” for facial augmentation deserves reconsideration. Autologous grafts remain biologically unmatched in many situations , but they also introduce donor-site morbidity, longer operative times, limited tissue availability, and biologic remodeling. Conversely, ePTFE offers predictable contour stability, elimination of donor-site harvest, controlled tissue integration, and relative ease of revision while accepting a different—and generally low—profile of implant-specific complications.⁵–⁸
Ultimately, successful facial augmentation depends less on choosing the most biologic material than on choosing the most appropriate material.
As surgeons continue to pursue increasingly individualized treatment strategies, the future of facial augmentation will likely be defined not by adherence to historical hierarchies of implant materials but by evidence-based selection tailored to each patient’s anatomy, reconstructive needs, and long-term goals.
Author’s Note
The purpose of this article is not to advocate for ePTFE implants over autologous tissue in every circumstance. Rather, it encourages surgeons to critically evaluate long-standing assumptions regarding facial augmentation and to recognize that contemporary biomaterials have evolved substantially over the past three decades. Both autologous tissue and ePTFE remain valuable components of the facial surgeon’s reconstructive armamentarium, and optimal outcomes depend upon thoughtful patient selection, meticulous surgical technique, and matching the implant material to the clinical indication.
References
- Maas CS, Gnepp DR, Bumpous JM. Expanded polytetrafluoroethylene (Gore-Tex soft-tissue patch) in facial augmentation. Arch Otolaryngol Head Neck Surg. 1993;119(9):1008-1014.
- Rohrich RJ, Ahmad J. Rhinoplasty and autogenous grafting: current concepts in cartilage grafting. Plast Reconstr Surg. (Review article.)
- Daniel RK. Diced cartilage grafts in rhinoplasty surgery. Plast Reconstr Surg. Various publications.
- Maas CS, Eriksson T, McCalmont TH, et al. Evaluation of expanded polytetrafluoroethylene as a soft-tissue filling substance: an analysis of design-related implant behavior using a porcine model. Plast Reconstr Surg. 1998;102(5):1307-1314.
- Godin MS, Waldman SR, Johnson CM Jr. The use of expanded polytetrafluoroethylene (Gore-Tex) in rhinoplasty: a 6-year experience. Arch Otolaryngol Head Neck Surg. 1995;121:1131-1136.
- Wang J, Liu Y, Zhao J, et al. The use of expanded polytetrafluoroethylene in depressed deformities of the face. Exp Ther Med. 2016;12(4):2369-2374.
- Kauke-Navarro M, Wetzels JWG, et al. A systematic review of implant materials for facial reconstructive and aesthetic surgery. Front Surg. 2025.
- Wee JH, Park MH, Oh S, Jin HR. Complications associated with autologous rib cartilage use in rhinoplasty: a meta-analysis. JAMA Facial Plast Surg. 2015;17(1):49-55.
- Flowers RS. Expanded polytetrafluoroethylene augmentation of deep nasolabial creases. Arch Otolaryngol Head Neck Surg. 1995;121:1007-1013.
- Hamdan US, Rohrich RJ, et al. Treatment of infected facial implants. Semin Plast Surg. 2016;30(2):87-92.
- Lee JM, Lee JS, Kim DK, et al. Antibacterial effects of the povidone-iodine vacuum impregnation technique in expanded polytetrafluoroethylene augmentation rhinoplasty. Ear Nose Throat J. 2016;95(7):E16-E22.
- Park JH, et al. Decontamination techniques for expanded polytetrafluoroethylene implants in rhinoplasty. Korean J Otorhinolaryngol Head Neck Surg. 2009.
- Wetzels JWG, et al. Balancing beauty and science: facial implant materials in reconstructive and aesthetic surgery. Front Surg. 2024.
- Fried MP, Lawson W. Tissue response to Gore-Tex facial implants. Arch Otolaryngol. 1983.
- Shin YS, et al. Long-term outcomes of augmentation rhinoplasty using expanded polytetrafluoroethylene: a 10-year clinical experience. Korean J Otorhinolaryngol Head Neck Surg.